Is It Epstein Barr Virus Reactivation?

Did You Know?
- Epstein-Barr Virus (EBV): 90% of us are carriers.
- EBV is part of the herpes virus family.
- EBV is known as a promiscuous virus.
- One study showed that 80% of Hashimoto Thyroiditis cases correlated with EBV and, EBV can enter the thyroid gland.
EBV Reactivation
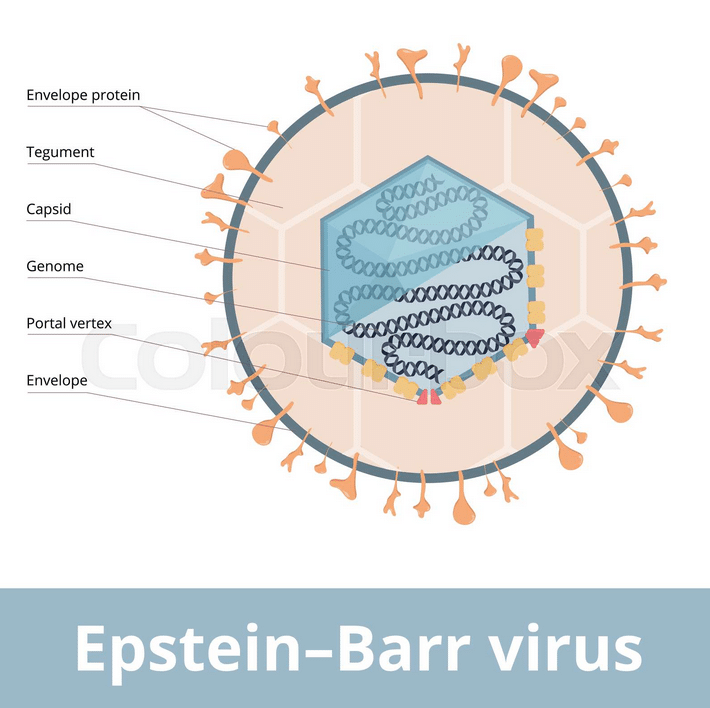
Epstein-Barr Virus (EBV), also known as human herpesvirus 4, is a common virus that belongs to the herpesvirus family. It is one of the most widespread viruses globally and infects a large portion of the population. EBV is known for causing a range of illnesses, including infectious mononucleosis (Mono) for most, but some people may acquire this without the initial onset of Mono. In some, EBV acquisition may go unnoticed as it can cause a mild or asymptomatic infection.
In today’s article, I’ll discuss EBV reactivation, what this particular virus can trigger in the body and how to test and treat this.
Acquiring EBV as Mono:
Mono, also referred to as the “kissing disease,” is a common illness caused by the Epstein-Barr Virus. It’s primarily transmitted through the exchange of saliva, which is why it’s associated with activities like kissing, sharing drinks, or close contact with an infected person. Once the virus enters the body, it initially infects the cells in the throat and mouth, particularly the B-cell lymphocytes (a type of white blood cell).
The symptoms of Mono can vary but often include fatigue, fever, sore throat, swollen lymph nodes, and general malaise, all lasting two weeks. In some cases, the symptoms can be severe, leading to a prolonged period of fatigue and discomfort.
EBV Reactivation:
After the initial infection, the immune system works to control the virus. However, EBV doesn’t completely leave the body after the acute illness subsides. Instead, it remains latent (dormant) in certain cells, particularly B cells. In most cases, the immune system keeps the latent virus in check (or dormant), preventing it from causing illness.
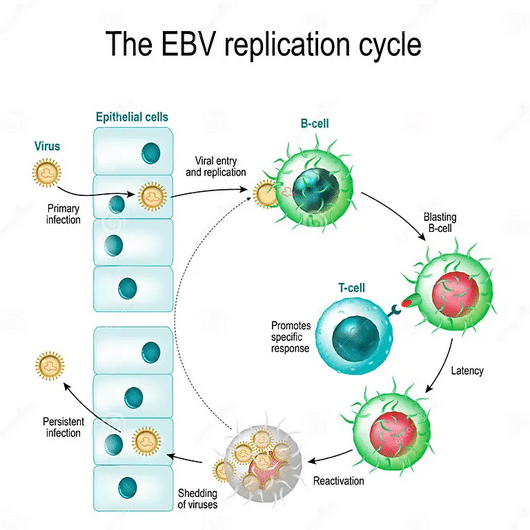
However, under certain conditions, such as when the immune system is weakened or stressed, the virus can reactivate and start replicating again. This can lead to a recurrence of symptoms, although typically milder than the initial Mono infection. Reactivations are more common in individuals with weakened immune systems, or individuals under severe stress.
In my clinical practice, I find that most people are under severe stress, and they don’t even know it. They know that they have some stress of course. Yet, they don’t appreciate the scope of their stress and what exactly this stress load is doing to their health.
- If you are a caregiver to a family member, you are under severe stress.
- If you have chronic health problems, you are under severe stress.
- If you aren’t sleeping enough, you’re always on the go, work life is stressful, and, you were alive during the last three years with COVID, lockdowns, worry and the political atmosphere, you’re likely under severe stress.
When you’re under constant stress, your immune system becomes dysregulated and this can lead to EBV reactivation.
Testing for EBV
There are four titers (measure of load of antibodies present in blood) to test for EBV. Most mainstream medical doctors do not believe that Epstein Barr Virus can chronically recur. Yet, if you do a quick search of Pubmed.gov for ‘EBV Reactivation’ you’ll find well over 2000 studies on EBV reactivation.
What I see clinically, is that the majority of doctors will discard any positive titers (unless EBV VCA IgM is positive) as a past infection. However, the issue with IgM, is that it’s rarely caught on blood work with a reactivation. At initial Mononucleosis EBV infection, IgM does increase, but only for a few weeks to a month. Then it drops. With reactivation, most people don’t seek out immediate help from their doctor. They instead equate their symptoms to not sleeping well, or extra stress, or not eating well and simply think that their symptoms will eventually pass. Most people don’t go to their doctor for a few months after onset of symptoms.
The Four EBV Titers and Their Elevation Timing and Duration
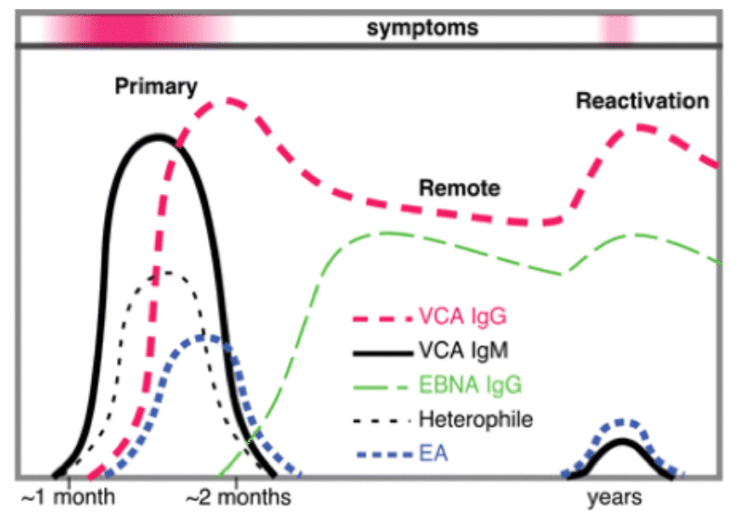
- EBV VCA IgM (Viral Capsid antigen) – rises and falls within a few weeks to month of Mono onset.
- EBV EA IgG (Early Antigen) – rises and falls within the first few months of Mono onset and reactivation.
- EBV VCA IgG (Viral Capsid antigen) – rises after a month of Mono onset and stays *elevated.
- EBV EBNA IgG (Epstein Barr Nuclear antigen) – rises after a month of Mono onset and stays *elevated.
- Heterophile: (in the chart) refers to the marker tested for Mononucleosis onset. Heterophile is not positive when EBV reactivates.
*Stays elevated means, that IgG levels will remain positive for life. However, when IgG levels are over 6 times the normal level, this can be reactivation.
To properly diagnose EBV, I look for EBV EA IgG to be positive, and either/ or EBV VCA IgG and EBV EBNA IgG to be 6+ times the normal level.
When requesting labs through your doctor, the titers MUST include EBV EA IgG. Even if you ask for this, be prepared to find that the panel run will not include this titer. That’s because most of the standard titer lab sets exclude EBV EA IgG.
Note that the goal of recovering from reactivated EBV is to get the virus to go back into a “dormant” state. EBV will never truly be eradicated from your body.
When a virus reactivates, other viruses can reactivate. That’s why it’s best to run a viral panel that assesses for overall viral load. Reactivation of EBV is also known to happen with COVID-19.
The viral panel that I run clinically looks at cytomegalovirus, EBV, additional herpes viruses and Strep A. The assessment for diagnosis is looking at a pooled marker; EBV IgM & IgG titers are combined in this lab.
Test Now with the Viral Infections Panel
Promiscuous Virus
Epstein-Barr Virus (EBV), is known as a promiscuous virus due to its ability to navigate the human body with a remarkable knack for infiltrating multiple organs and glands. This ability to infiltrate the body brings both challenges and consequences that reverberate through the body’s intricate systems. Let’s explore which organs and glands are susceptible to EBV infiltration and examine the effects it can have on the body.
EBV’s Multifaceted Reach:
EBV’s promiscuity lies in its ability to infiltrate and infect diverse cell types within the body. While its primary target is B lymphocytes, EBV doesn’t stop there. It can infiltrate a range of organs and glands, including but not limited to:
- Lymph Nodes: As a virus that initially targets B lymphocytes, EBV often causes swelling of lymph nodes, a hallmark symptom of infections like infectious mononucleosis (Mono)[1].
- Salivary Glands: EBV’s transmission via saliva underscores its affinity for the salivary glands. Infection can lead to swelling of these glands and contribute to the transmission of the virus[2].
- Thymus: The thymus, a critical organ for immune cell development, isn’t immune to EBV’s reach. The virus has been detected in thymic tissue[3].
- Spleen: EBV’s ability to infiltrate spleen tissue can contribute to splenomegaly, or an enlarged spleen, often observed in Mono cases[4].
- Liver: EBV can affect liver function, leading to symptoms like jaundice. It’s been implicated in some cases of hepatitis[5].
- Central Nervous System (CNS): Although rare, EBV can infiltrate the CNS, potentially leading to neurological symptoms[6].
- Brain: The blood-brain barrier typically restricts the entry of pathogens into the brain. However, research has indicated that EBV possesses the ability to breach this barrier and enter the central nervous system (CNS)[7]. This capacity for CNS infiltration is a topic of ongoing investigation, and while rare, it highlights the virus’s potential to impact neurological health [8].
- Thyroid: While the exact mechanisms are not fully elucidated, the virus’s capability to infiltrate thyroid cells potentially carries implications for thyroid health and autoimmune thyroid disorders like Hashimoto’s thyroiditis[9].
Consequences of EBV Infiltration into the Thyroid
The consequences of EBV’s infiltration into these organs and glands are diverse and complex. Let’s look at EBV and thyroid as an example.
In 2015, a significant contribution to the understanding of the relationship between Epstein-Barr Virus (EBV) and autoimmune thyroid diseases emerged from a Polish study[10]. This study examined the presence of EBV in two common autoimmune thyroid conditions: Hashimoto’s thyroiditis and Graves’ disease.
The study’s findings revealed compelling insights into the prevalence of EBV infection in these conditions. Among the cases of Hashimoto’s thyroiditis, a substantial 80.7% demonstrated the presence of EBV, while in Graves’ disease cases, the presence was noted in 62.5% of instances.
The implications of these findings are far-reaching. The study postulated that the high prevalence of EBV infection in both Hashimoto’s and Graves’ diseases hints at a potential etiological role of EBV in autoimmune thyroiditis.
Potential Mechanisms: Researchers have proposed several mechanisms by which EBV infection might contribute to the development of Hashimoto’s thyroiditis:
- Molecular Mimicry: EBV infection could trigger an immune response that inadvertently targets thyroid tissue due to molecular similarities between EBV antigens and thyroid proteins[11].
- Immune Dysregulation: EBV has the ability to modulate the immune response and immune cells. A dysregulated immune response might contribute to autoimmune disorders like Hashimoto’s[12].
- Genetic Susceptibility: Some studies suggest that individuals with certain genetic predispositions may be more susceptible to both EBV infection and autoimmune thyroid conditions[13].
- EBV Triggers Host Immune System Response: EBV infection can draw the attention of the immune system to target EBV in the thyroid gland and in doing so, the immune system may start attacking self, leading to autoimmune thyroiditis[14].
Could then, the attack on the thyroid gland by the immune system, be the correct immune response? The answer is yes, however, at what cost? According to this study, the result is activation of autoimmune condition.
If you went to your doctor with symptoms and the labs identified a hypothyroid condition and this was treated, but your symptoms haven’t resolved, I highly recommend running a viral panel to rule out EBV and viral load. Test Now with the Viral Infections Panel
Epstein-Barr Virus (EBV) is a common virus that can cause various illnesses, including infectious mononucleosis (Mono). It is primarily transmitted through the exchange of saliva and infects B lymphocytes in the throat and mouth. After the initial infection, EBV can remain dormant in the body and reactivate under certain conditions, leading to recurrent symptoms. While recurrent infections can occur, they are generally milder than the primary Mono infection.
EBV is known as a promiscuous virus. When it reactivates, it can move among the body’s organs and glands through the infected B-cells and this includes the thyroid gland. It is currently theorized that over 90% of Hashimoto’s cases (autoimmune thyroid are theorized to be EBV).
The Polish study published in 2015 offers valuable insights into the intricate interplay between EBV and autoimmune thyroid diseases. By highlighting the prevalence of EBV in Hashimoto’s thyroiditis and Graves’ disease cases and establishing a connection between specific markers, the study suggests a potential etiological role for EBV in the development of autoimmune thyroiditis. The proposed mechanism involving EBV’s influence on the initiation of autoimmune thyroiditis sheds light on a previously unexplored avenue in the realm of thyroid health research.
- Cohen, J. I. (2015). Epstein-Barr virus vaccines. Clinical & Experimental Immunology, 160(3), 328-332.
- Niedobitek, G. (2000). Epstein-Barr virus infection in the pathogenesis of nasopharyngeal carcinoma. Molecular Pathology, 53(5), 248-254.
- Cirocchi, R., D’Andrea, V., Amato, B., Renzi, C., & Grassi, V. (2007). Epstein-Barr virus thymic infection. World Journal of Surgical Oncology, 5(1), 63.
- Cohen, J. I. (2015). Epstein-Barr virus vaccines. Clinical & Experimental Immunology, 160(3), 328-332.
- Cohen, J. I. (2015). Epstein-Barr virus vaccines. Clinical & Experimental Immunology, 160(3), 328-332.
- Sergerie, Y., Boivin, G., Gosselin, D., Rivest, S., & Boivin, G. (2007). Presence of Epstein-Barr virus in the brain and spinal cord of elderly individuals. Journal of General Virology, 88(8), 2324-2330.
- Adamson, A. L., & Kenney, S. (2010). Epstein-Barr virus immediate-early protein BZLF1 is SUMO‐1 modified and disrupts promyelocytic leukemia bodies. Journal of Virology, 84(3), 1550-1558.
- Sengupta, S., & Kumar, P. (2014). The multifaceted role of Epstein–Barr virus (EBV) in cancer. In Tumor Virology (pp. 123-159). Springer.
- Sergerie, Y., Boivin, G., Gosselin, D., Rivest, S., & Boivin, G. (2007). Presence of Epstein-Barr virus in the brain and spinal cord of elderly individuals. Journal of General Virology, 88(8), 2324-2330.
- Kowalik, A., Słowińska-Klencka, D., Klencki, M., Wolska, M., Popko, K., Zebracka-Gala, J., … & Niedziela, M. (2015). High prevalence of Epstein-Barr virus infection in patients with Hashimoto’s thyroiditis and Graves’ disease. Autoimmunity, 48(3), 153-158.
- Burek, C. L., & Rose, N. R. (1999). Autoimmune thyroiditis and ROS. Autoimmunity Reviews, 18(2), 224-229.
- Strieder, T. G., Prummel, M. F., Tijssen, J. G., & Endert, E. (2003). Risk factors for and prevalence of thyroid disorders in a cross-sectional study among healthy female relatives of patients with autoimmune thyroid disease. Clinical Endocrinology, 59(3), 396-401.
- Tomer, Y., & Huber, A. (2009). The etiology of autoimmune thyroid disease: a story of genes and environment. Journal of Autoimmunity, 32(3-4), 231-239.
- Moss DJ, Burrows SR, Khanna R. EBV: immunobiology and host response. In: Arvin A, Campadelli-Fiume G, Mocarski E, et al., editors. Human Herpesviruses: Biology, Therapy, and Immunoprophylaxis. Cambridge: Cambridge University Press; 2007. Chapter 51.






